

SOUTH TAMPA THERAPY FREE RESOURCES BLOG

The Starved Brain: Why does your loved one with Anorexia think, feel, and act the way they do?
Literally Starving to get needs met. Self sabotage into self compassion. We can help.
The Starved Brain: Why does your loved one with Anorexia think, feel, and act the way they do?
If you have a loved one with Anorexia, you know more than anyone that eating disorders impact the entire family. It can feel like everything you know and have come to expect from your loved one changes overnight. I have had family members report to me:
“It’s like he is a whole different person”
“Is my precious happy girl still inside that body?”
“My wife has always been the life of the party. That’s one of the reasons I married her, now I can’t get her to leave the house”
It can be tremendously confusing and sometimes feelings of hopelessness emerge. That is very normal. It is scary. To understand these jarring changes, it is helpful to remember that Anorexia is a physical illness. It manifests, if not treated early, in significant weight loss and calorie restriction. Your loved one is acting, thinking, and feeling the way they are because of what research tells us about The Psychology of Hunger.
The Psychology of Hunger: The Starved Brain
The most notable study conducted the starved brain was undertaken in 1948 by Ancel Keys, called “The Biology of Human Starvation or popularly known as “The Minnesota Starvation Experiment.” The purpose of the experiment was to demonstrate how the body and mind are affected by not eating, or by restricting food. In this study, healthy young men were observed under normal conditions then exposed to caloric restriction (1570 calories a day for 6 months). After the semi-starvation period, they were rehabilitated with the purpose of determining the most successful form of nutritional rehabilitation. Such a study would never be conducted in modern research, but the results were foundational in shifting perceptions and guiding modern treatment interventions for Anorexia.
The Results
Below are the symptoms that were found at just 1570 calories a day for 6 months. *It is noteworthy that most sufferers of Anorexia eat far less than 1570 calories a day*
Physical: Less energy, reduced heart muscle mass, lower heart rate and blood pressure, headaches, decreased hormone levels, sensitivity to noise and light, a feeling of being cold all the time, loss of strength and greater fatigue and hair loss and dry skin.
Emotional and Cognitive changes: Depression, anxiety, irritability, increased mood fluctuations, intense and negative emotional reactions, decreased enthusiasm, reduced motivation, impaired concentration, problem solving and comprehension, increased rigidity, obsessional thinking, and reduced alertness.
Attitudes and behaviors related to food: Thinking about food all the time, eating very slow or very fast, increased hunger, unusual food routines and rituals, binge eating, increased use of condiments for flavor.
Social changes: Feeling more critical of others, withdrawn and isolated, loss of sense of humor, feelings of social inadequacy, neglect of personal hygiene and strained relationships.
These men had no previous mental health diagnosis, significant childhood trauma, or any health conditions that would skew the results in any meaningful way.
Implications
When working with sufferers and their family members I always share this study and pay special attention to highlight the results in the emotional/cognitive changes and social changes sections. I have seen the implications of this study reduce shame and destigmatize the individual suffering. I try to communicate that your loved one is still the same person you know; they are just experiencing the brains response to starvation. With appropriate nutritional rehabilitation and patience there is no reason to believe that most, if not all, of these symptoms will go away completely. The first step to treating Anorexia is weight restoration. Getting stuck in the “Why” vortex is tempting because the sufferer and family want to believe that if they knew why their loved one developed Anorexia it would give them the solution. Sometimes family members blame themselves: endlessly analyzing and hypothesizing about some unknown error they made. It is important to make sense of or peace with your loved one’s diagnosis but if there is anything you can do to support your loved one, it is to encourage them to seek nutritional rehabilitation first and foremost. I ask family members to avoid pathologizing their loved one. Going to therapy once a week while severely malnourished can be unfruitful because of the starved brain. A therapist role is to encourage motivation for recovery, educate and normalize Anorexia, and celebrate the little wins. Once your loved one is weight restored, the deeper work can be done from a healthy nourished brain. Should you be a family member of a sufferer in early stages of recovery, the primary take-away is to remind yourself and your loved that their brain is starving and the way they feel, think, and behave are survival responses. Remind them that it is not their fault, and it will not feel like this forever. Your loved one is not ‘CRAZY’ nor has their character or personality fundamentally changed they are just starving.
By Shaundra McGuire, MHCI
Book an appointment with Shaundra Mcguire:
https://SouthTampaTherapyBOOKAPPT.as.me/ShaundraMcguireMFTI
Additional resources for you and your loved one:
https://www.nationaleatingdisorders.org/
https://www.gaudianiclinic.com/videos-press
References:
https://eatingdisorders.dukehealth.org/education/resources/starvation-experiment

Healthy ways to Manage Stress and Anxiety
Stress and anxiety are emotions we often experience that cause us to feel a tightening in our body, making it harder to breathe, and bringing in negative thoughts. While experiencing these emotions from time to time is completely normal and serves a purpose, we can not allow these feelings to dictate our lives. This blog post will explore the different ways we can manage and control our stress and anxiety.
Take a minute to pause and think: When experiencing stress and anxiety it is important to pause and understand why we are feeling this way. Doing so will allow us to pinpoint what is causing our stress and anxiety and help us figure out what to do next.
Breathing exercises/ meditation: Take a minute to purposefully control your breathing. Doing so will allow you to focus on one specific thing and slow down you’re thinking and your heart rate. Meditation does the same exact thing; it allows you to intentionally think about one thing without outside distractions and other thoughts.
Get up and move: Sometimes the best way to release any pent-up anxiety and stress is to get up and move. Whether it be going for a walk/ run, going to the gym, or swimming, getting out that extra energy can help us release any unresolved or stress-inducing thoughts or emotions.
Getting enough sleep & eating a well-balanced meal: I know, I know you hear it often enough. Get 8 hours of sleep and eat healthily. As much as we don’t like to hear it, getting the right amount of sleep and eating right fuels our body with the right kind of energy that will propel us through the day. When we have that healthy energy we are less likely to become anxious and stressed because our bodies are charged and primed to take on difficult tasks.
Accept that you cannot control everything: We as humans have the instinct to want to be in control of everything in our lives, that way nothing can stop us from what we want to do. Unfortunately, it is not realistic for us to be able to control everything. We have to take accountability for ourselves, but also realize that there is a variable of life that will constantly be unknown. That can be scary to understand that we don’t have control of a lot of things, but we can find solace in the things we can control, ourselves and our reactions.
Positive Self-Talk: One great way to manage our stress and anxiety is to work on our positive self-talk. When we hear those negative voices making us anxious, we can combat them with positive thoughts or accept that we made a mistake and move forward without getting stuck in that negative loop. A great way to combat those anxious thoughts is to think about all the things you are grateful for at that moment or what you have done great so far today. Doing so will not only get rid of those negative thoughts, but it will also boost your self-esteem.
Self-Care: Finally, keeping up with your own self-care regimen will help keep your stress and anxiety at bay. We often think of self-care as taking bubble baths and relaxing, but it isn’t only that. Self-care is about evaluating where you are and what your needs are and taking the time to meet those needs. Just like getting enough sleep and eating a balanced meal, self-care allows your body to recharge with the right kind of energy you need to get through the day without being stressed out and anxious.
Although we may never be able to get rid of stress and anxiety, we have the tools to better manage those feelings. Utilizing these tools will allow us to not become overwhelmed when we feel anxious and stressed out. Instead, we will be better able to analyze where these feelings are coming from and meet whatever need is not being meant.
By Bailey McConnell, MFTI
Resources
Powell, T., & Enright, S. (2015). Anxiety and stress management. Routledge.
Ratanasiripong, P., Park, J. F., Ratanasiripong, N., & Kathalae, D. (2015). Stress and anxiety management in nursing students: Biofeedback and mindfulness meditation. Journal of Nursing Education, 54(9), 520-524.
Tips to Manage Anxiety and Stress. Anxiety & Depression Association of America. (2021, September 28). Retrieved from https://adaa.org/tips
Van den Bergh, O. (2021). Principles and practice of stress management. Guilford Publications.
Book an appointment with Bailey McConnell, MFTI
https://SouthTampaTherapyBOOKAPPT.as.me/BaileyMcConnellMFTI

3 Way to Help Your Anxious Child
Watching your child struggle with anxiety can be heartbreaking and leave parents feeling lost and helpless about how to help their child. On top of feeling helpless, as the anxiety grows, you may find that you are sacrificing more and more to lessen its effects on your child. The good news is that anxiety is treatable and there are things parents can do to help their kids overcome it.
Here are three tips for helping your child through their anxiety:
Don’t avoid it
Anxiety grows bigger and stronger when we allow it to tell us what we can and cannot do. It might relieve the distress and uncomfortable feelings for a day, but it only reinforces the idea that avoiding what makes someone anxious is the only way to overcome it.
For many parents, when their child is in distress, their natural instinct is to try to help their child by taking what is causing that distress away. When dealing with anxiety, it makes sense why encouraging a child to face their fears and subjecting them to discomfort is counterintuitive for a lot of parents. However, supporting your child through doing scary things and not helping them avoid what triggers their anxiety, only works to make the anxiety bigger.
Offer Support
Another way to respond when your child’s anxiety shows up is to offer them support through it. Support in this sense involves two parts. First, acknowledge what your child is feeling. Let them know that you see it is hard for them and empathize with what they are going through. Second, instill confidence in them that no matter what happens you know they will get through it. We may not be able to assure them that everything will be okay but they can make it through the hard feelings.
If your child is suffering from severe anxiety and is not ready to face their fears, start small and introduce them to the idea that avoidance only makes the anxiety worse. Starting a conversation with them about how they think they should start facing the anxiety is a great way to get them involved.
Find a therapist
Finding a therapist who is CBT informed can make a huge difference in the life of an anxious child or teen. Cognitive Behavioral Therapy allows a child to be gradually exposed to things that trigger their anxiety in a safe setting. Children can also learn techniques for identifying their anxious feelings and valuable coping skills for when they come up.
Therapists can also work with parents to focus on behavioral changes that parents can make to increase their child’s tolerance to anxiety. Parents and therapists work to gradually decrease accommodations that the family may be making that are not only making the anxiety bigger, but may also be causing a lot of stress to the family as a whole.
By Amanda Kohl, MCHI
SCHEDULE AN APPOINTMENT with Amanda Kohl, MCHI: https://SouthTampaTherapyBOOKAPPT.as.me/AmandaKohlMHCI

Understanding Fight, Flight, Freeze and the Fawn Trauma Response
The most well-known responses to trauma are the fight, flight, or freeze responses. However, there is a fourth possible response, the so-called fawn response. Flight includes running or fleeing the situation, fight is to become aggressive, and freeze is to literally become incapable of moving or making a choice.
The fawn response involves immediately moving to try to please a person to avoid any conflict. This is often a response developed in childhood trauma, where a parent or a significant authority figure is the abuser. Children go into a fawn-like response to attempt to avoid the abuse, which may be verbal, physical, or sexual, by being a pleaser. In other words, they preemptively attempt to appease the abuser by agreeing, answering what they know the parent wants to hear, or by ignoring their personal feelings and desires and do anything and everything to prevent the abuse.
Another possible response to trauma.
Most people have some level of awareness of PTSD, particularly as it applies to people returning from the war zones in the Middle East. PTSD was also evident in other soldiers returning from battle in the past, but there was limited recognition of the changes brought about by severe trauma in these earlier wars.
Today, research into the brain's response to trauma has created an awareness of PTSD across a wide range of life events. This includes seeing and experiencing the horrors of war, but also for first responders, victims of crime, and people exposed to single incidents of trauma or ongoing trauma throughout their life.
The most well-known responses to trauma are the fight, flight, or freeze responses. However, there is a fourth possible response, the so-called fawn response. Flight includes running or fleeing the situation, fight is to become aggressive, and freeze is to literally become incapable of moving or making a choice.
The fawn response involves immediately moving to try to please a person to avoid any conflict. This is often a response developed in childhood trauma, where a parent or a significant authority figure is the abuser. Children go into a fawn-like response to attempt to avoid the abuse, which may be verbal, physical, or sexual, by being a pleaser. In other words, they preemptively attempt to appease the abuser by agreeing, answering what they know the parent wants to hear, or by ignoring their personal feelings and desires and do anything and everything to prevent the abuse.
Over time, this fawn response becomes a pattern. Individuals carry this behavior pattern into their adult relationships, including their professional and personal interactions.
Recognizing the Fawn Response
As the fawn response is developed early in childhood, it can be difficult for an individual to recognize it is occurring. However, there are some key signs that the fawn response is in use when:
· You look to others for how you feel in a relationship or a situation
· It is difficult to identify your feelings, even when you are alone
· You often feel like you have no identity
· You are constantly trying to please the people in your life
· At the first sign of conflict, your first instinct is to appease the angry person
· You ignore your own beliefs, thoughts, and truths and accept those of the people around you
· You may experience unusual emotional responses when issues do not involve people of importance in your life. This could include emotional outbursts at strangers or sudden sadness throughout the day.
· You feel self-anger and guilt some or most of the time
· Saying no to those around you is a challenge
· You are overwhelmed at times but take on more if asked
· You lack boundaries and are often taken advantage of in relationships
· You are uncomfortable or threatened when asked to give an opinio
The fawn response is often not discussed in PTSD as it may be seen as simply a part of the personality of the individual. However, it goes beyond a collaborative and non-competitive personality.
Individuals with the fawn response pattern can be targeted by those who are narcissistic or those with a desire to control and manipulate people around them. In these situations, the fawn response creates a dangerous cycle with the narcissist demanding more and more and the individual with PTSD feeling greater levels of anger, guilt, and self-reproach for giving their emotional and physical all to the partner.
Getting Help
Trauma, including PTSD, can be treated effectively through therapeutic interventions. Working closely with a therapist trained in the treatment of PTSD is essential to understand the cause of the trauma and to process the past to be able to move forward.
Through therapy, individuals who use this type of response as their default way to deal with others can learn effective strategies to create and maintain boundaries, to talk about their feelings and emotions, and to learn how to interact with others without feeling the need to constantly please.
The 4Fs: A Trauma Typology in Complex PTSD
By Pete Walker
http://pete-walker.com/fourFs_TraumaTypologyComplexPTSD.htm
This paper describes a trauma typology for differentially diagnosing and treating Complex Post Traumatic Stress Disorder. This model elaborates four basic defensive structures that develop out of our instinctive Fight, Flight, Freeze and Fawn responses to severe abandonment and trauma (heretofore referred to as the 4Fs). Variances in the childhood abuse/neglect pattern, birth order, and genetic predispositions result in individuals "choosing" and specializing in narcissistic (fight), obsessive/compulsive (flight), dissociative (freeze) or codependent (fawn) defenses. Many of my clients have reported that psychoeducation in this model has been motivational, deshaming and pragmatically helpful in guiding their recovery.
Individuals who experience "good enough parenting" in childhood arrive in adulthood with a healthy and flexible response repertoire to danger. In the face of real danger, they have appropriate access to all of their 4F choices. Easy access to the fight response insures good boundaries, healthy assertiveness and aggressive self-protectiveness if necessary. Untraumatized individuals also easily and appropriately access their flight instinct and disengage and retreat when confrontation would exacerbate their danger. They also freeze appropriately and give up and quit struggling when further activity or resistance is futile or counterproductive. And finally they also fawn in a liquid, "play-space" manner and are able to listen, help, and compromise as readily as they assert and express themselves and their needs, rights and points of view.
Those who are repetitively traumatized in childhood however, often learn to survive by over-relying on the use of one or two of the 4F Reponses. Fixation in any one 4F response not only delimits the ability to access all the others, but also severely impairs the individual's ability to relax into an undefended state, circumscribing him in a very narrow, impoverished experience of life. Over time a habitual 4F defense also "serves" to distract the individual from the accumulating unbearable feelings of her current alienation and unresolved past trauma.
Complex PTSD as an Attachment Disorder
Polarization to a fight, flight, freeze or fawn response is not only the developing child's unconscious attempt to obviate danger, but also a strategy to purchase some illusion or modicum of attachment. All 4F types are commonly ambivalent about real intimacy because deep relating so easily triggers them into painful emotional flashbacks (see my article in The East Bay Therapist (Sept/Oct 05): "Flashback Management in the Treatment of Complex PTSD". Emotional Flashbacks are instant and sometimes prolonged regressions into the intense, overwhelming feeling states of childhood abuse and neglect: fear, shame, alienation, rage, grief and/or depression. Habituated 4F defenses offer protection against further re-abandonment hurts by precluding the type of vulnerable relating that is prone to re-invoke childhood feelings of being attacked, unseen, and unappreciated.
Fight types avoid real intimacy by unconsciously alienating others with their angry and controlling demands for the unmet childhood need of unconditional love; flight types stay perpetually busy and industrious to avoid potentially triggering interactions; freeze types hide away in their rooms and reveries; and fawn types avoid emotional investment and potential disappointment by barely showing themselves - by hiding behind their helpful personas, over-listening, over-eliciting or overdoing for the other - by giving service but never risking real self-exposure and the possibility of deeper level rejection. Here then, are further descriptions of the 4F defenses with specific recommendations for treatment. All types additionally need and benefit greatly from the multidimensional treatment approach described in the article above, and in my East Bay Therapist article (Sept/Oct06): "Shrinking The Inner Critic in Complex PTSD", which describes thirteen toxic superegoic processes of perfectionism and endangerment that dominate the psyches of all 4F types in varying ways.
The Fight Type and the Narcissistic Defense
Fight types are unconsciously driven by the belief that power and control can create safety, assuage abandonment and secure love. Children who are spoiled and given insufficient limits (a uniquely painful type of abandonment) and children who are allowed to imitate the bullying of a narcissistic parent may develop a fixated fight response to being triggered. These types learn to respond to their feelings of abandonment with anger and subsequently use contempt, a toxic amalgam of narcissistic rage and disgust, to intimidate and shame others into mirroring them and into acting as extensions of themselves. The entitled fight type commonly uses others as an audience for his incessant monologizing, and may treat a "captured" freeze or fawn type as a slave or prisoner in a dominance-submission relationship. Especially devolved fight types may become sociopathic, ranging along a continuum that stretches between corrupt politician and vicious criminal.
TX: Treatable fight types benefit from being psychoeducated about the prodigious price they pay for controlling others with intimidation. Less injured types are able to see how potential intimates become so afraid and/or resentful of them that they cannot manifest the warmth or real liking the fight type so desperately desires. I have helped a number of fight types understand the following downward spiral of power and alienation: excessive use of power triggers a fearful emotional withdrawal in the other, which makes the fight type feel even more abandoned and, in turn, more outraged and contemptuous, which then further distances the "intimate", which in turn increases their rage and disgust, which creates increasing distance and withholding of warmth, ad infinitem. Fight types need to learn to notice and renounce their habit of instantly morphing abandonment feelings into rage and disgust. As they become more conscious of their abandonment feelings, they can focus on and feel their abandonment fear and shame without transmuting it into rage or disgust - and without letting grandiose overcompensations turn it into demandingness.
Unlike the other 4Fs, fight types assess themselves as perfect and project the inner critic's perfectionistic processes onto others, guaranteeing themselves an endless supply of justifications to rage. Fight types need to see how their condescending, moral-high-ground position alienates others and perpetuates their present time abandonment. Learning to take self-initiated timeouts at the first sign of triggering is an invaluable tool for them to acquire. Timeouts can be used to accurately redirect the lion's share of their hurt feelings into grieving and working through their original abandonment, rather than displacing it destructively onto current intimates. Furthermore, like all 4F fixations, fight types need to become more flexible and adaptable in using the other 4F responses to perceived danger, especially the polar opposite and complementary fawn response described below. They can learn the empathy response of the fawn position - imagining how it feels to be the other, and in the beginning "fake it until they make it." Without real consideration for the other, without reciprocity and dialogicality, the real intimacy they crave will remain unavailable to them.
The Flight Type and the Obsessive-Compulsive Defense
Flight types appear as if their starter button is stuck in the "on" position. They are obsessively and compulsively driven by the unconscious belief that perfection will make them safe and loveable. As children, flight types respond to their family trauma somewhere along a hyperactive continuum that stretches between the extremes of the driven "A" student and the ADHD dropout running amok. They relentlessly flee the inner pain of their abandonment and lack of attachment with the symbolic flight of constant busyness.
When the obsessive/compulsive flight type is not doing, she is worrying and planning about doing. Flight types are prone to becoming addicted to their own adrenalization, and many recklessly and regularly pursue risky and dangerous activities to keep their adrenalin-high going. These types are also as susceptible to stimulating substance addictions, as they are to their favorite process addictions: workaholism and busyholism. Severely traumatized flight types may devolve into severe anxiety and panic disorders.
TX: Many flight types are so busy trying to stay one step ahead of their pain that introspecting out loud in the therapy hour is the only time they find to take themselves seriously. While psychoeducation is important and essential to all the types, flight types particularly benefit from it. Nowhere is this truer than in the work of learning to deconstruct their overidentification with the perfectionistic demands of their inner critic. Gently and repetitively confronting denial and minimization about the costs of perfectionism is essential, especially with workaholics who often admit their addiction to work but secretly hold onto it as a badge of pride and superiority. Deeper work with flight types - as with all types -gradually opens them to grieving their original abandonment and all its concomitant losses. Egosyntonic crying is an unparalleled tool for shrinking the obsessive perseverations of the critic and for ameliorating the habit of compulsive rushing. As recovery progresses, flight types can acquire a "gearbox" that allows them to engage life at a variety of speeds, including neutral. Flight types also benefit from using mini-minute meditations to help them identify and deconstruct their habitual "running". I teach such clients to sit comfortably, systemically relax, breathe deeply and diaphragmatically, and ask themselves questions such as: "What is my most important priority right now?", or when more time is available: "What hurt am I running from right now? Can I open my heart to the idea and image of soothing myself in my pain?" Finally, there are numerous flight types who exhibit symptoms that may be misperceived as cyclothymic bipolar disorder; I address this issue at length in my article: "Managing Abandonment Depression in Complex PTSD".
The Freeze Type and the Dissociative Defense
Many freeze types unconsciously believe that people and danger are synonymous, and that safety lies in solitude. Outside of fantasy, many give up entirely on the possibility of love. The freeze response, also known as the camouflage response, often triggers the individual into hiding, isolating and eschewing human contact as much as possible. This type can be so frozen in retreat mode that it seems as if their starter button is stuck in the "off" position. It is usually the most profoundly abandoned child - "the lost child" - who is forced to "choose" and habituate to the freeze response (the most primitive of the 4Fs). Unable to successfully employ fight, flight or fawn responses, the freeze type's defenses develop around classical dissociation, which allows him to disconnect from experiencing his abandonment pain, and protects him from risky social interactions - any of which might trigger feelings of being reabandoned. Freeze types often present as ADD; they seek refuge and comfort in prolonged bouts of sleep, daydreaming, wishing and right brain-dominant activities like TV, computer and video games. They master the art of changing the internal channel whenever inner experience becomes uncomfortable. When they are especially traumatized or triggered, they may exhibit a schizoid-like detachment from ordinary reality.
TX: There are at least three reasons why freeze types are the most difficult 4F defense to treat. First, their positive relational experiences are few if any, and they are therefore extremely reluctant to enter the relationship of therapy; moreover, those who manage to overcome this reluctance often spook easily and quickly terminate. Second, they are harder to psychoeducate about the trauma basis of their complaints because, like many fight types, they are unconscious of their fear and their torturous inner critic. Also, like the fight type, the freeze type tends to project the perfectionistic demands of the critic onto others rather than the self, and uses the imperfections of others as justification for isolation. The critic's processes of perfectionism and endangerment, extremely unconscious in freeze types, must be made conscious and deconstructed as described in detail in my aforementioned article on shrinking the inner critic. Third, even more than workaholic flight types, freeze types are in denial about the life narrowing consequences of their singular adaptation. Because the freeze response is on a continuum that ends with the collapse response (the extreme abandonment of consciousness seen in prey animals about to be killed), many appear to be able to self-medicate by releasing the internal opioids that the animal brain is programmed to release when danger is so great that death seems immanent. The opioid production of the collapse or extreme freeze response can only take the individual so far however, and these types are therefore prone to sedating substance addictions. Many self-medicating types are often drawn to marijuana and narcotics, while others may gravitate toward ever escalating regimes of anti-depressants and anxiolytics. Moreover, when they are especially unremediated and unattached, they can devolve into increasing depression and, in worst case scenarios, into the kind of mental illness described in the book, I Never Promised You A Rose Garden.
The Fawn Type and the Codependent Defense
Fawn types seek safety by merging with the wishes, needs and demands of others. They act as if they unconsciously believe that the price of admission to any relationship is the forfeiture of all their needs, rights, preferences and boundaries. They often begin life like the precocious children described in Alice Miler's The Drama Of The Gifted Child, who learn that a modicum of safety and attachment can be gained by becoming the helpful and compliant servants of their parents. They are usually the children of at least one narcissistic parent who uses contempt to press them into service, scaring and shaming them out of developing a healthy sense of self: an egoic locus of self-protection, self-care and self-compassion. This dynamic is explored at length in my East Bay Therapist article (Jan/Feb2003): "Codependency, Trauma and The Fawn Response" (see www.pete-walker.com). TX. Fawn types typically respond well to being psychoeducated in this model. This is especially true when the therapist persists in helping them recognize and renounce the repetition compulsion that draws them to narcissistic types who exploit them. Therapy also naturally helps them to shrink their characteristic listening defense as they are guided to widen and deepen their self-expression. I have seen numerous inveterate codependents finally progress in their assertiveness and boundary-making work, when they finally got that even the thought of expressing a preference or need triggers an emotional flashback of such intensity that they completely dissociate from their knowledge of and ability to express what they want. Role-playing assertiveness in session and attending to the stultifying inner critic processes it triggers helps the codependent build a healthy ego. This is especially true when the therapist interprets, witnesses and validates how the individual as a child was forced to put to death so much of her individual self. Grieving these losses further potentiates the developing ego.
Trauma Hybrids
There are, of course, few pure types. Most trauma survivors are hybrids of the 4F's. There are for instance, three subsets of the fawn type: the fawn-fight (the smothering-mother type) who coercively or manipulatively takes care of others, who smother loves them into conforming with her view of who they should be; the fawn-flight type who workaholically makes herself useful to others (the "model" secretary) in the vein of her favorite role model Mother Theresa; and the fawn-freeze type who numbingly surrenders herself to scapegoating or to a narcissist's need to have a target for his rageaholic releases (the "classic" domestic violence victim).Space in this article only allows for the description of two other common hybrids: the Fight/Fawn and the Flight/Freeze.
The Fight/Fawn, perhaps the most relational hybrid and most susceptible to love addiction, combines two opposite but magnetically attracting polarities of relational style - narcissism and codependence. This defense is sometimes misdiagnosed as borderline because the individual's flashbacks trigger a panicky sense of abandonment and a desperation for love that causes her to dramatically split back and forth between fighting and clawing for love and cunningly or flatteringly groveling for it. This type is different than the fawn/fight in that the narcissistic defense is typically more in ascendancy. The fight/fawn hybrid is also distinct from a more common condition where an individual acts like a fight type in one relationship while fawning in another (the archetypal henpecked husband who is a tyrant at work), and from the many "nice" mildly codependent people who have critical masses where they will eventually get fed up and blow up about injustice and exploitation. The borderline-like fight/fawn type however may dramatically vacillate back and forth between these two styles many times in a single interaction.
The Flight/Freeze type is the least relational and most schizoid hybrid. This type avoids his feelings and potential relationship retraumatization with an obsessive-compulsive/ dissociative "two-step" that severely narrows his existence. The flight/freeze cul-de-sac is more common among men, especially those traumatized for being vulnerable in childhood, and those who subsequently learned to seek safety in isolation or "intimacy-lite" relationships. Many non-alpha type males gravitate to the combination of flight and freeze defensiveness stereotypical of the information technology nerd - the computer addict who workaholically focuses for long periods of time and then drifts off dissociatively into computer games. Many sex addicts also combine flight and freeze in a compulsive pursuit of a sexual pseudo-intimacy. When in flight mode, they obsessively scheme to "get" sex and/or compulsively pursue and/or engage in it; when in freeze mode, they drift off into a right brain sexual fantasy world that is often fueled by an addictive use of pornography; and even during real time sexual interaction, they often engage more with their idealized fantasy partners than with their actual partner.
Self-Assessment. Readers may find it informative to self-assess their own hierarchical use of the 4F responses. They can try to determine their dominant type and hybrid, and think about what percentage of their time is spent in each type of 4F activity. Finally, all 4Fs progressively recover from the multidimensional wounding of complex ptsd as mindfulness of learned trauma dynamics increases, as the critic shrinks, as dissociation decreases, as childhood losses are effectively grieved, as the healthy ego matures into a user-friendly manager of the psyche, as the life narrative becomes more egosyntonic, as emotional vulnerability creates authentic experiences of intimacy, and as "good enough" safe attachments are attained. Furthermore, it is also important to emphasize that recovery is not an all-or-none phenomenon, but rather a gradual one marked by decreasing frequency, intensity and duration of flashbacks.



Depression: What It Is and What to Do about It (Part I)
This is the first of a two-part series on depression. In this issue, I will explore what depression is and what causes it. In the next issue, I will describe how depression is treated and prevented. If you or someone close to you suffers from depression, it is important to educate yourself about it and seek treatment from qualified mental health professionals.
Depression is a serious illness, not a harmless part of life. It is a complex disorder with a variety of causes. It is never caused by just one thing. It may be the result of a mix of factors, including genetic, chemical, physical, and sociological. It is also influenced by behavior patterns learned in the family and by cognitive distortions.
Depression affects millions of people in this country. It is always troubling, and for some people it can be disabling. Depression is more than just sadness or "the blues." It can have an impact on nearly every aspect of a person's life. People who suffer from depression may experience despair and worthlessness, and this can have an enormous impact on both personal and professional relationships. In this newsletter, I will describe many of the factors that may cause depression, and I will explore strategies for preventing it.
Depression Is Pervasive
When a person suffers from depression, it can affect every part of his or her life, including one's physical body, one's behavior, thought processes, mood, ability to relate to others, and general lifestyle.
Symptoms of Depression
People who are diagnosed with clinical depression have a combination of symptoms from the following list:
· Feelings of hopelessness, even when there is reason to be hopeful
· Fatigue or low energy
· Much less interest or pleasure in most regular activities
· Low self-esteem
· Feeling worthless
· Excessive or inappropriate guilt
· Lessened ability to think or concentrate
· Indecisiveness
· Thinking distorted thoughts; having an unrealistic view of life
· Weight loss or gain without dieting
· Change in appetite
· Change in sleeping patterns
· Recurrent thoughts of death
· Suicidal thoughts
· A specific plan for committing suicide
· A suicide attempt
· Feelings of restlessness or being slowed down
When a person is suffering from depression, these symptoms cause significant distress or impairment in social, occupational, or other important areas of functioning. This means that the person's family and social relationships, as well as work life, are impaired.
When a person is suffering from depression, symptoms such as these are not the result of a chronic psychotic disorder, substance abuse, general medical condition, or bereavement.
Grief, Sadness, and Depression
Depression may include feelings of sadness, but it is not the same as sadness. Depression lasts much longer than sadness. While depression involves a loss of self-esteem, grief, disappointment and sadness do not. People who are depressed function less productively. People who are sad or disappointed continue to function.
Depression and Socioeconomic Factors
Depression does not seem to be related to ethnicity, education, income, or marital status. It strikes slightly more women than men. Some researchers believe that depression strikes more often in women who have a history of emotional and sexual abuse, economic deprivation, or are dependent on others. There seems to be a genetic link; depression is more common among parents, children, and siblings of people who are diagnosed with depression. The average age at the onset of a depressive episode is the mid-20s. People born more recently are being diagnosed at a younger age.
Physical Causes
Many physicians believe that depression results from a chemical imbalance in the brain. They often prescribe antidepressant medication, and many people find relief as a result. However, there is no reliable test to identify such a chemical imbalance. It is unknown whether life experiences cause mood changes, which create changes in brain chemistry, or whether it works in reverse.
Depression may be associated with physical events such as other diseases, physical trauma, and hormonal changes. A person who is depressed should always have a physical examination as part of the assessment process to determine the role of physical causes.
Signs That Professional Treatment Is Needed
If you or someone you know is depressed and exhibits any of the following signs, it is extremely important to seek the assistance of a medical or mental health professional.
1. Thinking about death or suicide. This is always dangerous and you should see a professional therapist immediately.
2. When symptoms of depression continue for a long time, you may need professional help. Acute responses to events are normal, but they should not last beyond a reasonable time.
3. Your ability to function is impaired by your depression. Seek help before your life situation deteriorates to a serious level.
4. You have become so isolated that you have no one with whom to check reality. Seek out someone to share your thoughts and feelings with.
5. Depressive symptoms have become severe.
In my next newsletter, I will discuss the treatment and prevention of depression.

Why Am I So Anxious?
Why Am I So Anxious?
Fact: You Cannot Be Anxious and Relaxed At The Same Time! Therefore, the antidote to anxiety = relaxation...
Every human feels anxiety on occasion; it is a part of life. All of us know what it is like to feel worry, nervousness, fear, and concern. We feel nervous when we have to give a speech, go for a job interview, or walk into our boss's office for the annual performance appraisal. We know it's normal to feel a surge of fear when we unexpectedly see a photo of a snake or look down from the top of a tall building. Most of us manage these kinds of anxious feelings fairly well and are able to carry on with our lives without much difficulty. These feelings don't disrupt our lives.
But millions of people (an estimated 15% of the population) suffer from devastating and constant anxiety that severely affects their lives, sometimes resulting in living in highly restricted ways. These people experience panic attacks, phobias, extreme shyness, obsessive thoughts, and compulsive behaviors. The feeling of anxiety is a constant and dominating force that disrupts their lives. Some become prisoners in their own homes, unable to leave to work, drive, or visit the grocery store. For these people, anxiety is much more than just an occasional wave of apprehension.
Types of Anxiety Disorders
An anxiety disorder affects a person's behavior, thoughts, feelings, and physical sensations. The most common anxiety disorders include the following:
Social anxiety or social phobia is a fear of being around other people. People who suffer from this disorder always feel self-conscious around others. They have the feeling that everyone is watching them and staring at them, being critical in some way. Because the anxiety is so painful, they learn to stay away from social situations and avoid other people. Some eventually need to be alone at all times, in a room with the door closed. The feeling is pervasive and constant and even happens with people they know.
People who have social anxiety know that their thoughts and fears are not rational. They are aware that others are not actually judging or evaluating them at every moment. But this knowledge does not make the feelings disappear.
Panic disorder is a condition where a person has panic attacks without warning. According to the National Institutes of Mental Health, about 5% of the adult American population suffers from panic attacks. Some experts say that this number is actually higher, since many people experience panic attacks but never receive treatment.
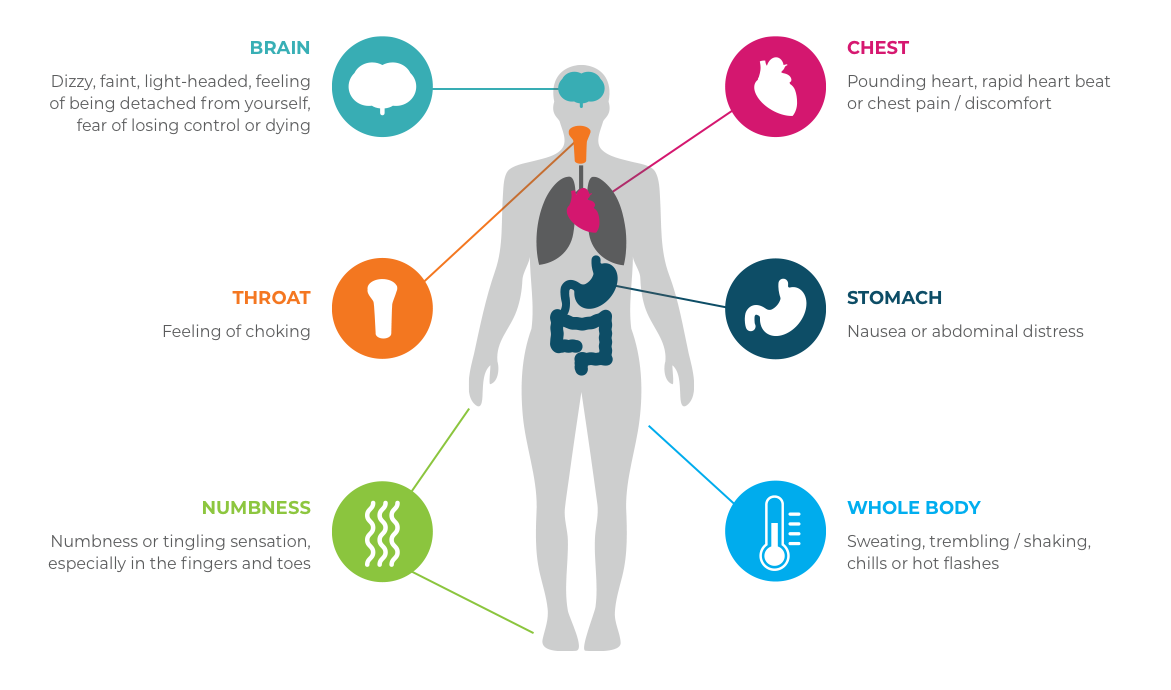
Common symptoms of panic include:
· Racing or pounding heart
· Trembling
· Sweaty palms
· Feelings of terror
· Chest pains or heaviness in the chest
· Dizziness and lightheadedness
· Fear of dying
· Fear of going crazy
· Fear of losing control
· Feeling unable to catch one's breath
· Tingling in the hands, feet, legs, or arms
A panic attack typically lasts several minutes and is extremely upsetting and frightening. In some cases, panic attacks last longer than a few minutes or strike several times in a short time period.
A panic attack is often followed by feelings of depression and helplessness. Most people who have experienced panic say that the greatest fear is that the panic attack will happen again.
Many times, the person who has a panic attack doesn't know what caused it. It seems to have come "out of the blue." At other times, people report that they were feeling extreme stress or had encountered difficult times and weren't surprised that they had a panic attack.
Generalized anxiety disorder is quite common, affecting an estimated 3 to 4% of the population. This disorder fills a person's life with worry, anxiety, and fear. People who have this disorder are always thinking and dwelling on the "what ifs" of every situation. It feels like there is no way out of the vicious cycle of anxiety and worry. The person often becomes depressed about life and their inability to stop worrying.
People who have generalized anxiety usually do not avoid situations, and they don't generally have panic attacks. They can become incapacitated by an inability to shut the mind off, and are overcome with feelings of worry, dread, fatigue, and a loss of interest in life. The person usually realizes these feelings are irrational, but the feelings are also very real. The person's mood can change from day to day, or even hour to hour. Feelings of anxiety and mood swings become a pattern that severely disrupts the quality of life.
People with generalized anxiety disorder often have physical symptoms including headaches, irritability, frustration, trembling, inability to concentrate, and sleep disturbances. They may also have symptoms of social phobia and panic disorder.
Other types of anxiety disorders include:
Phobia, fearing a specific object or situation.
Obsessive-compulsive disorder (OCD), a system of ritualized behaviors or obsessions that are driven by anxious thoughts.
Post-traumatic stress disorder (PTSD), severe anxiety that is triggered by memories of a past traumatic experience.
Agoraphobia, disabling fear that prevents one from leaving home or another safe place.
Treatment Options
Most people who suffer from anxiety disorders begin to feel better when they receive the proper treatment. It can be difficult to identify the correct treatment, however, because each person's anxiety is caused by a unique set of factors. It can be frustrating for the client when treatment is not immediately successful or takes longer than hoped for. Some clients feel better after a few weeks or months of treatment, while others may need a year or more. If a person has an anxiety disorder in combination with another disorder (such as alcoholism and depression), treatment is more complicated and takes longer.
While a treatment plan must be specifically designed for each individual, there are a number of standard approaches. Mental health professionals who specialize in treating anxiety most often use a combination of the following treatments. There is no single correct approach.
Cognitive Therapy
The client learns how to identify and change unproductive thought patterns by observing his or her feelings and learning to separate realistic from unrealistic thoughts.
Behavior Therapy
This treatment helps the client alter and control unwanted behavior. Systematic desensitization, a type of behavior therapy, is often used to help people with phobias and OCD. The client is exposed to anxiety-producing stimuli one small step at a time, gradually increasing his or her tolerance to situations that have produced disabling anxiety.
Relaxation Training
Many people with anxiety disorders benefit from self-hypnosis, guided visualization, and biofeedback. Relaxation training is often part of psychotherapy.
Medication
Antidepressant and antianxiety medications can help restore chemical imbalances that cause symptoms of anxiety. This is an effective treatment for many people, especially in combination with psychotherapy.
The treatment for an anxiety disorder depends on the severity and length of the problem. The client's willingness to actively participate in treatment is also an important factor. When a person with panic is motivated to try new behaviors and practice new skills and techniques, he or she can learn to change the way the brain responds to familiar thoughts and feelings that have previously caused anxiety.

How People Change
What Is Happiness?
If you are thinking about changing your life for the better, one way to start is by identifying your goals. You are probably hoping to find some version of happiness or emotional well-being. That might look like any combination of the following:
· A sense of freedom
· Self-esteem
· Self-confidence
· Happy to get up in the morning
· Working toward goals
· A sense of purpose in life
· Satisfying relationships
What Is Unhappiness?
If you are thinking about changing your life, you may be experiencing some combination of the following elements:
· Feeling sad, lethargic or depressed
· Feeling afraid
· Abusing or being addicted to alcohol or drugs
· Feeling lonely
· Anxiety
· Problems with relationships
· Not getting what you want in life; feeling frustrated in working toward goals
· Not caring enough to have goals
How Will You Change?
When you decide to change your life, try the following ideas.
1. Explore your feelings. Keep a journal, talk to a trusted friend, work with a professional counselor.
2. Envision your future. Write in a journal, make a collage, do a guided visualization, talk to a friend or counselor, research the possibilities.
3. Explore wishes and dreams. Keep a journal, talk to a trusted friend, work with a professional counselor.
4. Be open to new ideas. Take a class, travel, say yes to things you may have avoided in the past.
5. Look for kindred spirits. Avoid people who make you feel bad about yourself, seek out those who make you blossom, reach out to those with similar interests and dreams.
6. Try something different. Deliberately buy new items, try different brands, shop at different stores, do the opposite of what you usually do, see different movies, read different kinds of books and magazines.
7. Set goals and targets. Learn how to set useful goals, follow through, evaluate progress regularly, reward yourself for achievement.
8. Take one step at a time. Divide your goals into tiny pieces and do one small new thing each day, starting now.
9. Look for lessons. Remind yourself that experiences are not good or bad; they are simply lessons.
How to Overcome Your Resistance to Change
Have you ever noticed that when you think about changing your life, you feel resistant? Many people say that they not only feel resistant, but they actually do things to keep their lives familiar. They do things like start a diet and then eat a candy bar on the first day, or quit smoking and then sneak a puff.
There are some things you can do to make yourself less resistant. Here are six effective strategies:
1. Eliminate clutter. Clutter can be viewed as a sign of uncertainty. Accumulating "stuff" might be stopping you from committing to an important thing. If you keep a lot of half-started projects around, it makes it difficult to zero in on the really important things.
2. Start small. Thinking of your overall goal can be overwhelming. So manage your resistance by choosing one small part of it and attacking it today. Let's say your goal is to lose 20 pounds. That can certainly seem like an impossible thing to accomplish. It will seem more doable if you tell yourself, I'm going to lose five pounds by (date).
3. Disprove your disempowering beliefs. In Reinventing Your Life, authors Young and Klosko suggest that you identify the beliefs that keep you from succeeding. They offer a way to dispute those beliefs by asking, "Is there really an evidence today that this belief is true?" They suggest making a list of the evidence.
4. Remind yourself of all of your available options. You always have alternatives and the power to choose among them.
5. Take responsibility for what you want. Look for signs that you are blaming
your situation on others or not admitting past mistakes. Acknowledge them and move on.
6. Visualize the future. Author Barbara Sher suggests one way to do this: Write an imaginary press release about yourself. The date is today's date, two years in the future. The press release is announcing the most extraordinary event you can think of. It doesn't matter whether this event seems only vaguely possible to you. The important thing is that it is exciting to imagine.
When to Seek Professional Help
Sometimes it makes sense to find a professional counselor to work with as you work through the change process. Here are some ways to know when that would be appropriate:
1. You've tried several things but you still have the problem.
2. You want to find a solution sooner rather than later.
3. You have thoughts of harming yourself or others.
4. You have symptoms of depression, anxiety, or another disorder that are significantly interfering with your daily functioning and the quality of your life. For example, you have lost time from work, your relationships have been harmed, your health is suffering. These are signs that you may need the help of a trained, licensed professional.

Managing Perfectionism
Perfectionists aspire to be top achievers and do not allow themselves to make even a single mistake. They are always on the alert for imperfections and weaknesses in themselves and others. They tend to be rigid thinkers who are on the lookout for deviations from the rules or the norm.
Perfectionism is not the same as striving for excellence. People who pursue excellence in a healthy way take genuine pleasure in working to meet high standards. Perfectionists are motivated by self-doubt and fears of disapproval, ridicule, and rejection. The high producer has drive, while the perfectionist is driven.
Causes and Characteristics
Fear of failure and rejection. The perfectionist believes that she will be rejected or fail if she is not always perfect, so she becomes paralyzed and unable to produce or perform at all.
Fear of success. The perfectionist believes that if he is successful in what he undertakes, he will have to keep it up. This becomes a heavy burden-who wants to operate at such a high level all of the time?
Low self-esteem. A perfectionist's needs for love and approval tend to blind her to the needs and wishes of others. This makes it difficult or impossible to have healthy relationships with others.
Black-and-white thinking. Perfectionists see most experiences as either good or bad, perfect or imperfect. There is nothing in between. The perfectionist believes that the flawless product or superb performance must be produced every time. Perfectionists believe if it can't be done perfectly, it's not worth doing.
Extreme determination. Perfectionists are determined to overcome all obstacles to achieving success. This is also true of high achievers, but the perfectionist focuses only on the result of his efforts. He is unable to enjoy the process of producing the achievement. His relentless pursuit of the goal becomes his downfall because it often results in overwhelming anxiety, sabotaging his heroic efforts.
The Costs of Being a Perfectionist
Perfectionism always costs more than the benefits it might provide. It can result in being paralyzed with fear and becoming so rigid that a person is difficult to relate to. It can produce contradictory styles, from being highly productive to being completely nonproductive. Some examples of these costs include the following:
Low self-esteem. Just as low self-esteem is a cause of perfectionist behavior, it is also a result. Because a perfectionist never feels good enough about himself or his personal performance, he usually feels like a loser or a failure.
Gloominess. Since a perfectionist is convinced that it will be next to impossible to achieve most goals, she can easily develop a negative attitude.
Depression. Perfectionists often feel discouraged and depressed because they are driven to be perfect but know that it is impossible to reach the ideal.
Guilt. Perfectionists never think they handle things well. They often feel a sense of shame and guilt as a result.
Rigidity. Since perfectionists need to have everything meet an ideal, they tend to become inflexible and lack spontaneity.
Lack of motivation. A person who expects perfection may never try new behaviors or learn new skills because she thinks that she will never be able to do it well enough. At other times, she may begin the new behavior but give up early because she fears that she will never reach her goal.
Paralysis. Since most perfectionists have an intense fear of failure, they sometimes become immobilized and stagnant. Writers who suffer from writer's block are examples of the perfectionist's paralysis.
Obsessive behavior. When a person needs a certain order or structure in his life, he may become overly focused on details and rules.
Compulsive behavior. A perfectionist who feels like a failure or loser may medicate him- or herself with alcohol, drugs, food, shopping, sex, gambling, or other high-risk behaviors.
Eating disorders. Many studies have determined that perfectionism is a central issue for people who develop eating disorders.
The Perfectionist versus
The High Achiever
People produce many of their best achievements when they are striving to do their best. High achievers, like perfectionists, want to be better people and achieve great things. Unlike perfectionists, high achievers accept that making mistakes and risking failure are part of the achievement process-and part of being human.
Emotionally Healthy High Producers
You can be a high achiever without being a perfectionist. People who accomplish plenty and stay emotionally healthy tend to exhibit the following behaviors:
· Set standards that are high but achievable.
· Enjoy the process, not just the outcome.
· Recover from disappointment quickly.
· Are not disabled by anxiety and fear of failure.
· View mistakes as opportunities for growth and learning.
· React positively to constructive feedback.
Once you are aware of the ways by which you expect yourself to be perfect, you can start to change your behavior. In my next newsletter, I'll offer some tips to help you get started. Until then, begin the change process by thinking about which causes apply to you and writing down examples of these perfectionist behaviors as you observe them.